
A Patient Assessment Form serves as a vital tool in healthcare, ensuring structured evaluations and accurate recordkeeping. This guide covers its components, examples, and effective usage. Whether in hospitals, clinics, or physiotherapy sessions, it ensures patient data is well-organized and comprehensive. Incorporating details such as medical history, current conditions, and treatment plans, the Assessment Form enhances communication between healthcare providers and patients. It also supports compliance with regulatory standards. Discover the significance of this Patient Form and how it facilitates better outcomes for both patients and practitioners.
Download Patient Assessment Form Bundle
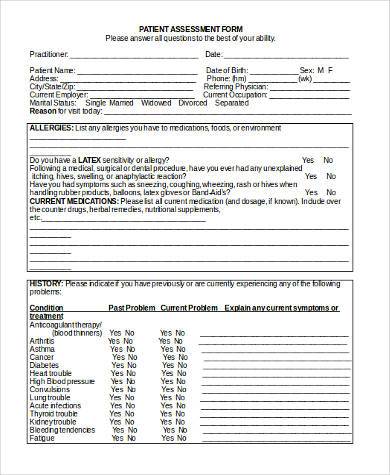
What is Patient Assessment Form?
A Patient Assessment Form is a structured document used in healthcare to evaluate and record a patient’s medical status. It includes fields for personal details, medical history, symptoms, and treatment plans. This essential tool streamlines patient care by ensuring consistent and thorough data collection. It aids healthcare professionals in understanding patient conditions, making informed decisions, and providing tailored treatment plans.
Patient Assessment Format
Patient Information
- Name: ____________________________
- Age: ____________________________
- Gender: ____________________________
- Contact Information: ____________________________
Medical History
- Known Allergies: ____________________________
- Current Medications: ____________________________
- Past Surgeries or Illnesses: ____________________________
- Family Medical History: ____________________________
Current Symptoms
- Main Complaint: ____________________________
- Duration: ____________________________
- Severity: ____________________________
- Other Symptoms: ____________________________
Assessment Notes
- Vital Signs: ____________________________
- Physical Examination Results: ____________________________
- Initial Diagnosis: ____________________________
- Recommended Tests: ____________________________
Healthcare Provider Information
- Provider’s Name: ____________________________
- Signature: ____________________________
- Date: ____________________________
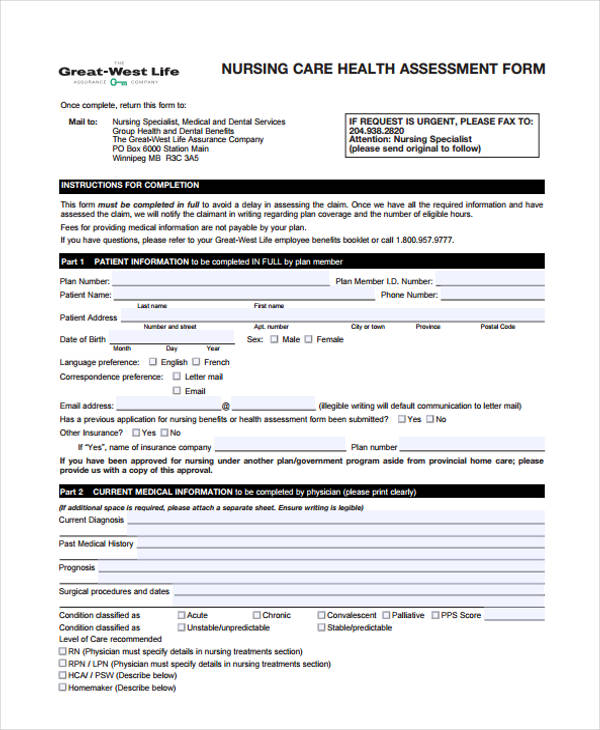
Patient Assessment Form For Nurses
A Patient Assessment Form for Nurses is designed to record patient health details during care. Similar to a School Assessment Form, it ensures thorough documentation of symptoms, medication, and nursing interventions for better outcomes.
Patient Assessment Form For Hospital
A Patient Assessment Form for Hospital use streamlines data collection for diagnostics and treatment. Like an Income Assessment Form, it ensures accurate information tracking to support patient care and financial accountability in medical settings.
Patient Assessment Form Physiotherapy
A Patient Assessment Form for Physiotherapy helps evaluate mobility, pain, and rehabilitation progress. Comparable to a Project Assessment Form, it structures therapy goals and tracks patient progress toward achieving optimal recovery outcomes.
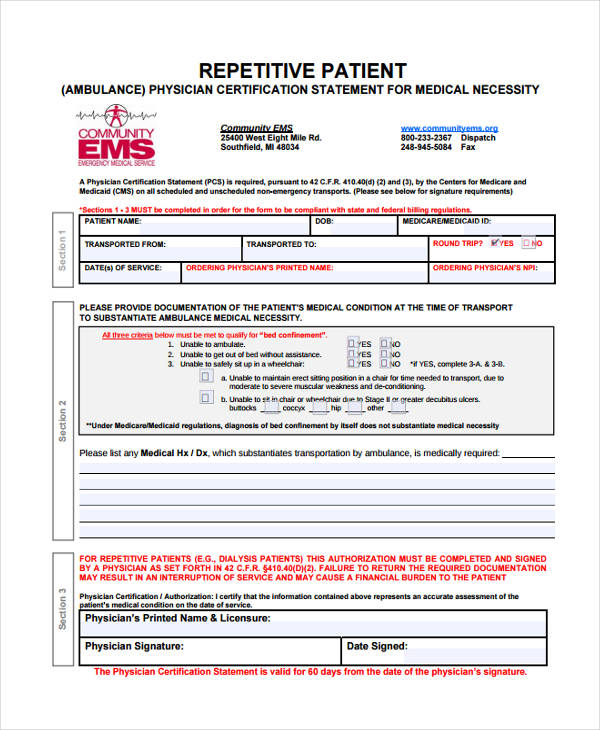
Emergency Patient Assessment Form
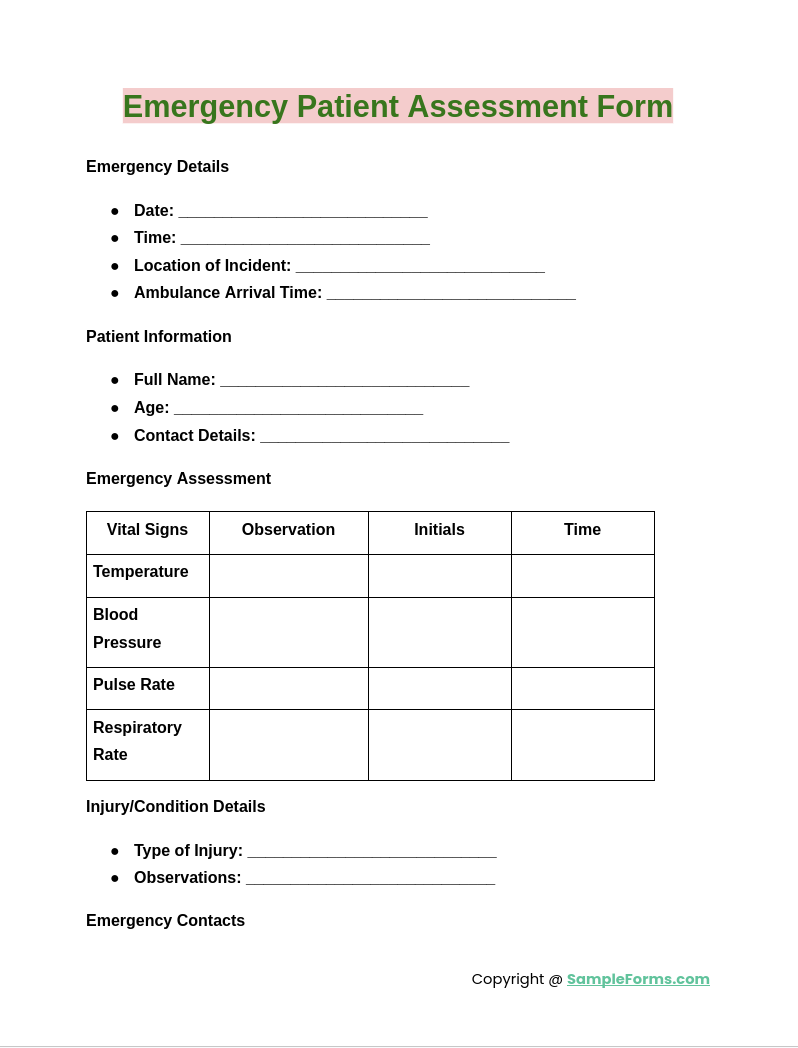
An Emergency Patient Assessment Form captures critical details for urgent care situations. Similar to a Financial Assessment Form, it ensures essential information is gathered quickly to enable prompt decision-making and effective emergency response.
Browse More Patient Assessment Forms
Nursing Patient Assessment
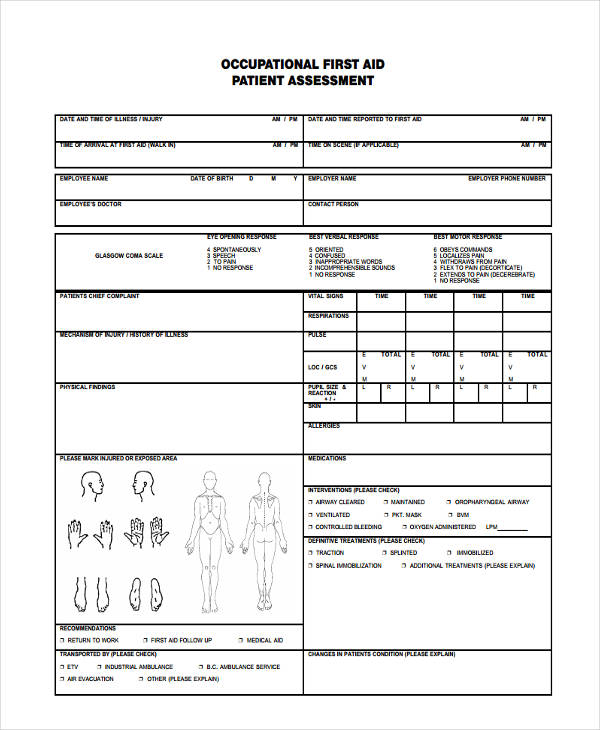
First Aid Patient
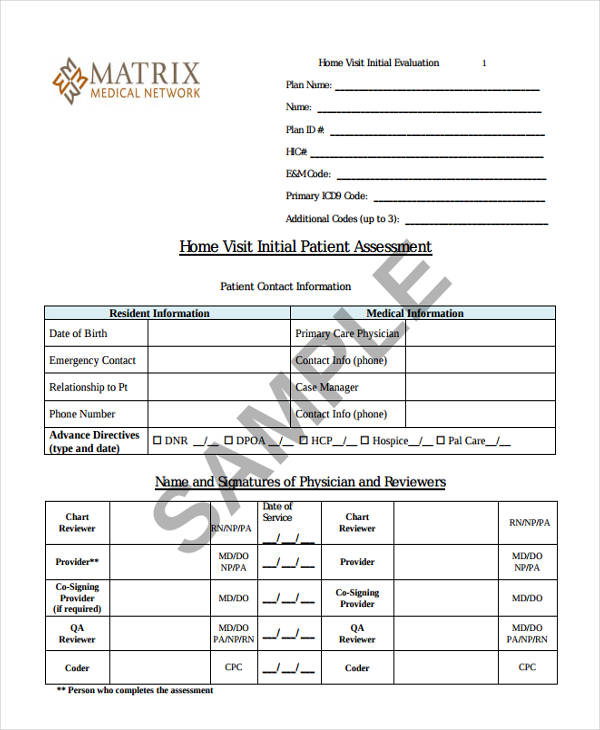
Initial Patient Assessment
Diabetes Patient Assessment

Emergency Patient
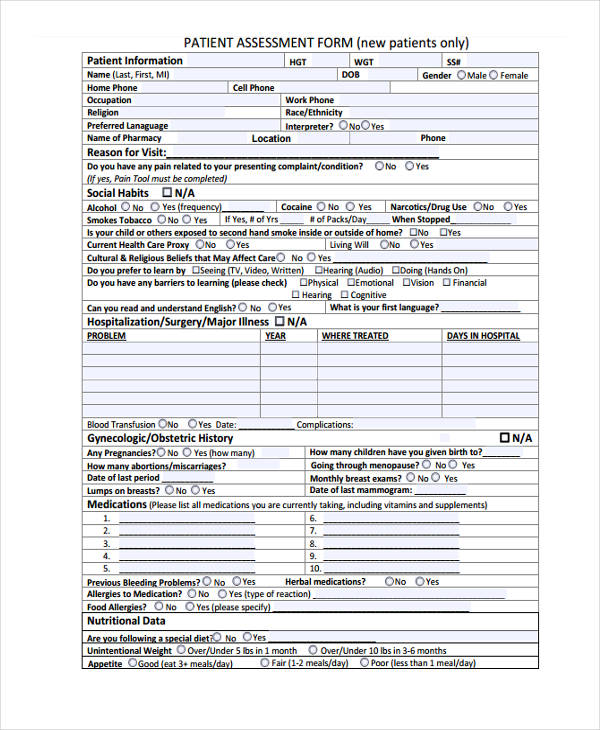
New Patient Assessment
Pediatric Patient

Repetitive Patient Assessment
Sample Patient Assessment
Patient Assessment Form in Word Format
Simple Patient Assessment Form

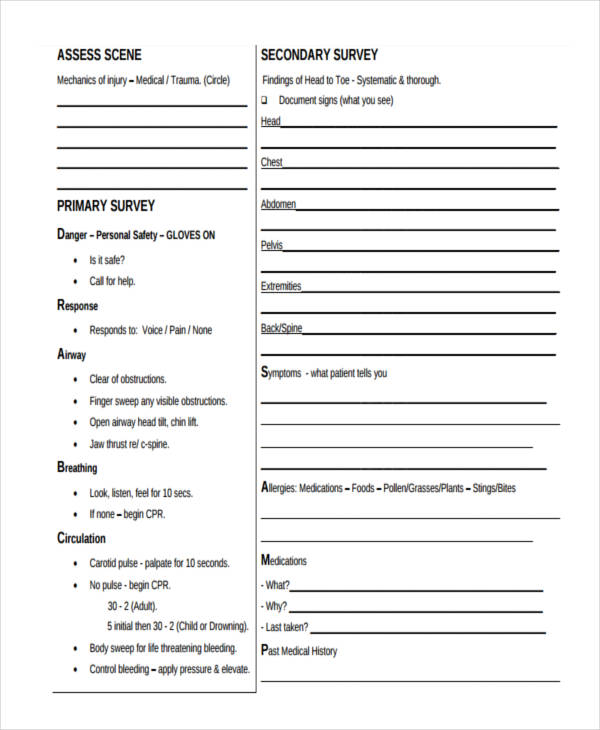
What are the steps in a patient assessment?
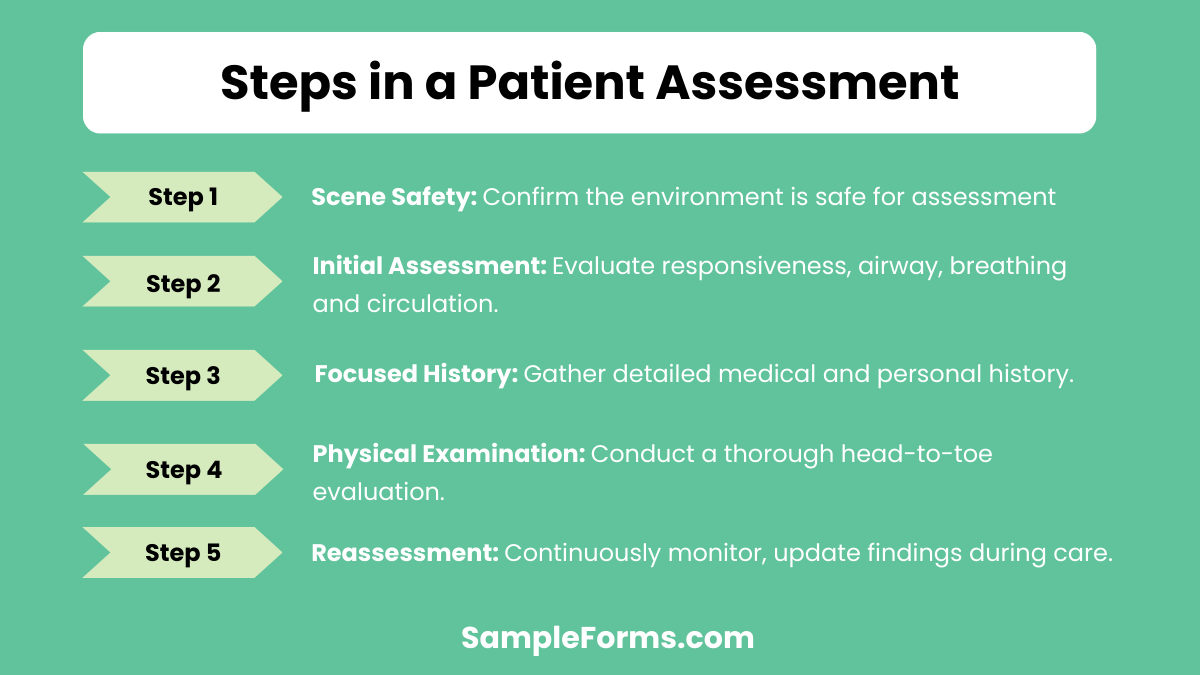
The five steps of patient assessment ensure methodical data collection and diagnosis for effective treatment.
- Scene Safety: Confirm the environment is safe for assessment, similar to a Client Assessment Form.
- Initial Assessment: Evaluate responsiveness, airway, breathing and circulation.
- Focused History: Gather detailed medical and personal history.
- Physical Examination: Conduct a thorough head-to-toe evaluation.
- Reassessment: Continuously monitor and update findings during care.
What primary actions make up patient assessment?

Four primary actions ensure a complete patient assessment, promoting safety and accuracy in healthcare delivery.
- Observation: Monitor patient appearance, posture, and behavior.
- Interviewing: Obtain detailed information through questions.
- Examination: Perform physical assessments, referencing tools like an Army Risk Assessment Form.
- Documentation: Record findings for continuity of care and analysis.
How do you write a patient assessment?
Writing a patient assessment involves gathering and documenting critical medical information. A structured approach ensures comprehensive evaluation and care coordination.
- Collect Patient Information: Include medical history, symptoms, and lifestyle factors using tools like a Capacity Assessment Form.
- Assess Symptoms: Document present symptoms and physical examination findings systematically.
- Record Vital Signs: Include temperature, blood pressure, and heart rate for baseline data.
- Evaluate Health Status: Use objective and subjective data to analyze the patient’s condition.
- Develop Treatment Plan: Coordinate findings into actionable steps for patient care.
What is the purpose of a patient assessment?
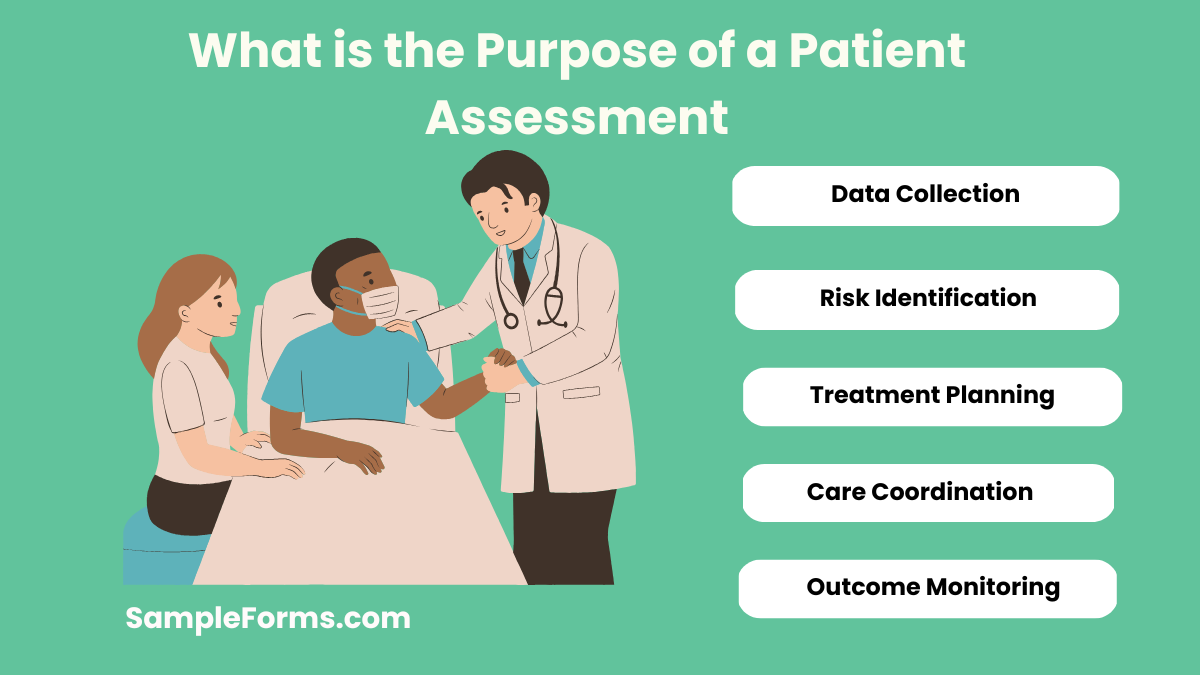
The purpose of a patient assessment is to identify health needs and provide accurate, individualized care, ensuring optimal treatment outcomes.
- Data Collection: Gather medical history and symptoms to inform diagnosis.
- Risk Identification: Assess risk factors using a Family Assessment Form.
- Treatment Planning: Develop strategies based on findings.
- Care Coordination: Enable collaboration among healthcare providers.
- Outcome Monitoring: Track progress to refine the care plan.
What is method to follow in patient assessment?
The method of patient assessment are essential for evaluating and addressing health concerns methodically.
- Patient Interaction: Build rapport and collect initial information using techniques like a Community Assessment Form.
- Health Evaluation: Conduct a physical examination to identify abnormalities.
- Diagnosis: Interpret findings to form a clinical diagnosis.
- Care Planning: Create and implement a comprehensive care strategy.
What is the most important part of patient assessment?
The most critical part of patient assessment is identifying life-threatening conditions promptly using a Physical Assessment Form to prioritize and stabilize care effectively.
Why do we need a patient assessment?
Patient assessments ensure accurate diagnosis and treatment plans while addressing overall health, incorporating tools like a Student Assessment Form for detailed evaluation.
What is the first step in patient assessment?
The first step is scene safety, ensuring the environment poses no danger, followed by initial evaluation using an Employee Assessment Form.
When should a patient be assessed?
Patients should be assessed during hospital admission, routine check-ups, or emergencies using tools like a Pre Training Assessment Form to determine immediate care needs.
How do you complete a patient assessment?
Complete patient assessments involve gathering history, physical examination, and diagnostics while recording findings in a Child Assessment Form to ensure thorough analysis.
What is the meaning of patient needs assessment?
Patient needs assessment identifies health requirements and resources, often documented with a Property Assessment Form for clarity and tailored care.
What is the purpose of completing a primary assessment on a patient?
Primary assessments focus on identifying urgent issues such as airway or circulation problems, leveraging tools like an Environmental Assessment Form.
What are the 5 C’s of patient care?
The 5 C’s include Communication, Compassion, Competence, Commitment, and Confidence, often evaluated using an Education Assessment Form for healthcare professionals.
How do you start a patient assessment?
Start by establishing rapport, gathering initial history, and using tools like an Assessment Form for Teacher for structured evaluation.
What is the purpose of a work assessment in healthcare?
A work assessment evaluates a patient’s ability to return to work or perform tasks, recorded with a Work Assessment Form for comprehensive insights.
The Patient Assessment Form is indispensable in medical documentation, facilitating effective patient care and decision-making. From capturing medical histories to treatment plans, it enhances communication and streamlines workflows. Whether for hospitals, clinics, or physiotherapy, its role in ensuring healthcare excellence is unmatched. Explore its usage and importance with detailed examples, including the Medicine Patient Intake Form, and elevate your healthcare processes.
Related Posts
-
Enquiry Form
-
FREE 5+ Recruiter Performance Review Forms in PDF | MS Word
-
Job Safety Observation Form
-
FREE 4+ Hazard Observation Forms in PDF
-
FREE 5+ Coach Observation Forms in PDF | MS Word
-
FREE 4+ Child Care Observation Forms in MS Word | PDF
-
FREE 4+ Child Observation Forms in PDF | MS Word
-
Preschool Observation Form
-
Student Observation Form
-
Peer Observation Form
-
Lesson Observation Form
-
Content Retention Through Assessment Form [ How to, Importance, Tips ]
-
The Importance of Risk Assessment and Safety Statement [ What Is, How to Conduct ]
-
Risk Assessments And Safety Statements Guidelines [ What Is, Process ]
-
Choosing Careers Through Self Assessment [ What Is, Ways ]